Written by Daniella Watson, King’s College London
Undernutrition contributes to up to 45% of child deaths in African countries. At the same time, child obesity rates have doubled between 2006 and 2016. More than 40% of women of reproductive age are anaemic. And 13.7% of infants have low weight at birth. Stunting in the African region is 30.7% – above the world average of 22%.
In 2020, over a fifth of Africa’s population faced hunger; 346.4 million people experience severe food insecurity; and 452 million experienced moderate food insecurity.
Nutrition programmes have been supporting families in Africa for decades. But many of these programmes have inconclusive results.
As health psychologists and behavioural scientists, we believe this is because the programmes don’t focus on fitting into families’ lives. Doing so would also make nutrition interventions sustainable. Understanding the behaviours of the people being targeted by nutrition programmes could improve their nutrition status.
Our recent research looked at the outcomes of studies that had behaviour change embedded within programmes to improve nutrition for mothers and children in sub-Saharan Africa. Our findings show that nutrition programmes that focus on family and community behaviour change have better health outcomes for mothers and children.
The World Health Organization has outlined the importance of behaviour change to support mother and child health and help address barriers in current nutrition programmes. Our study goes a step further to show how to use behaviour change models to design better nutrition programmes.
Behavioural science
Health psychologists and behavioural scientists developed the COM-B model. It suggests that a person’s Capability, Opportunity and Motivation can change their Behaviour. Our study showed that this model can be used to consider what is happening in the lives of people when designing nutrition interventions including what barriers there might be to eating healthy food.
“Capability” from the COM-B model refers to a person’s physical capability, such as their skill sets, and psychological capability, such as knowledge about a behaviour. If a person doesn’t know what foods to be eating to be healthy or doesn’t feel they have the skills to cook healthy foods, they can’t change the behaviour. Programmes need to support people to know what the healthy local foods are and how to cook these foods, potentially through community-led cooking demonstrations. Our findings show that simply educating people isn’t enough. Making lessons interactive and practical in people’s daily lives increases the likelihood of behaviour change.
“Opportunity” from the COM-B model refers to a person’s physical opportunities in their environment, and their social opportunities such as their family and wider community. For example, if communities don’t have apples and bananas growing in their environment, or for sale, then they simply won’t be able access these foods. Programmes therefore need to support the foods that are already available to buy in people’s environment. If possible, they should also support the wider community to grow food. The people around us influence what we do and what we eat. Programmes should try to encourage key community and family figures to support nutrition practices.
“Motivation” from the COM-B model refers to a person’s habits and things they do without realising it (automatic motivation). One of the habits or norms in many communities is to prioritise men, then children, to eat first. Women often get the leftovers, even when they are pregnant. This means that pregnant women don’t get the nutrients they need. Programmes need to work with women, men and wider communities to motivate them to prioritise women’s nutrition, while respecting culture and tradition. This would encourage reflective motivation where people can consciously make decisions about food within social structures.
Building nutrition programmes
When designing nutrition programmes, the best way to learn about people’s motivations is to ask them directly about the issues they are facing and the solutions they want. Once you know their issues and potential solutions, you can use behavioural science models such as the COM-B model to categorise the issues and solutions, and start designing programmes to address these gaps.
To go a step further, the same behavioural scientists also developed the Behaviour Change Wheel, which helps us to think of different methods.
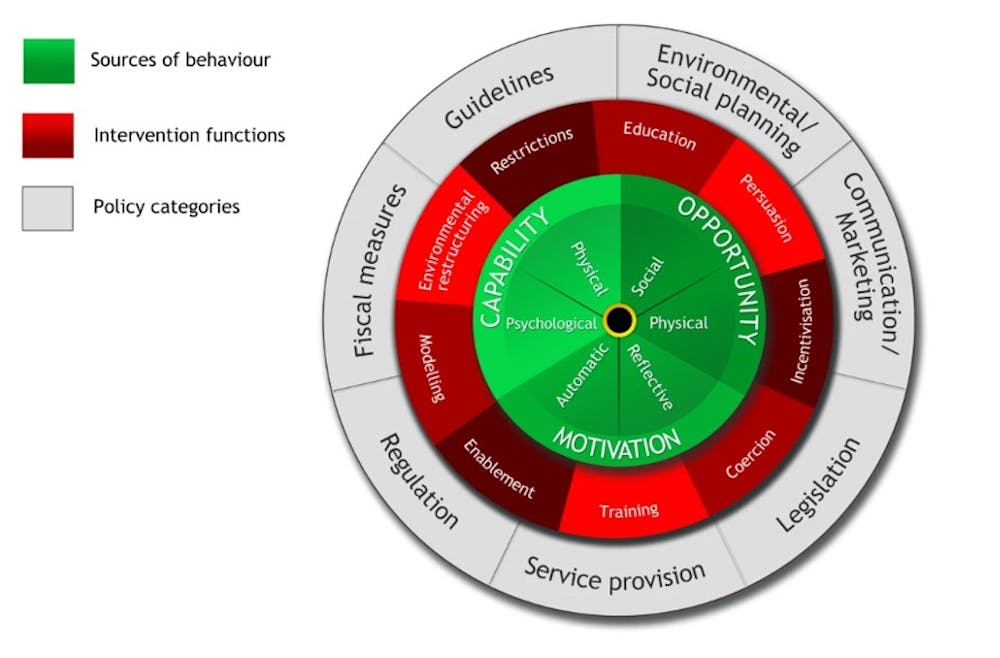
Our study shows that applying the Behaviour Change Wheel to nutrition programmes may also increase their impact. The wheel suggests:
- giving participants incentives
- using persuasive communication
- modelling healthy diets
- restructuring the environment
- educating on nutrition, in an interactive way
- supplying resources such as tools and seedlings (enablement)
- training communities in cooking or agricultural methods.
Using simple behavioural science models can help programmes to understand people’s lives and how to design nutrition interventions that directly benefit them, even when the funding ends.![]()
Daniella Watson, Postdoctoral Researcher and Health Psychologist, King’s College London
This article is republished from The Conversation under a Creative Commons license. Read the original article.
Photo by Emmanuel Ikwuegbu on Pexels
Relevant Agribook pages include “Food security“.